Although both types of diabetes cause high blood sugar and require careful monitoring, they differ in their causes, how they develop, treatment approaches, and possibilities for prevention. Understanding these differences helps improve disease management and avoid misconceptions.
1. Cause
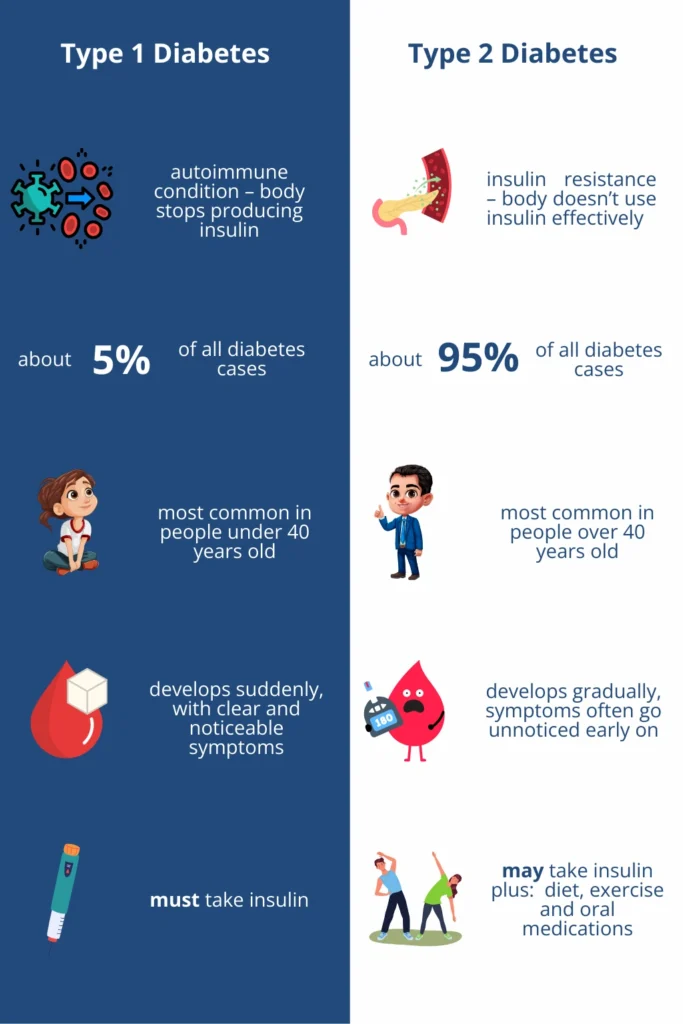
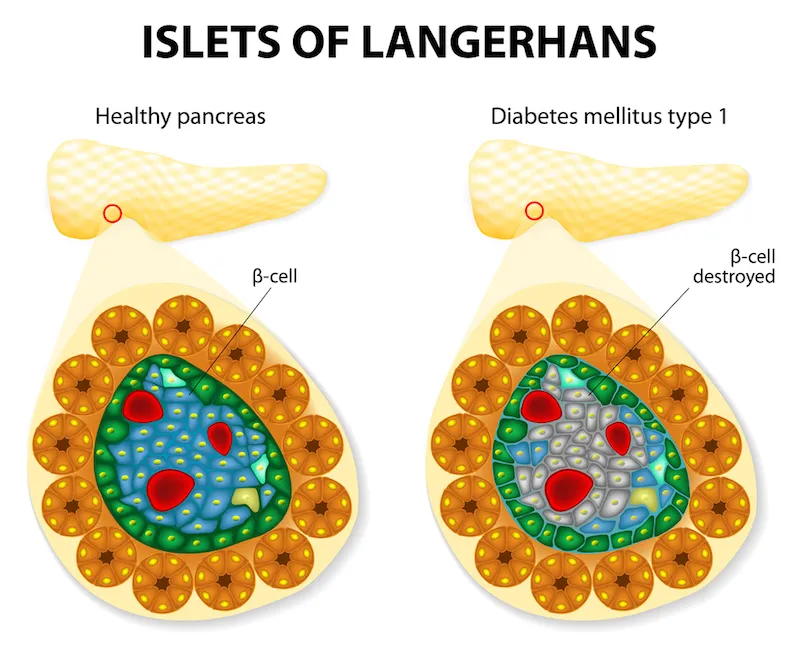
Type 1 Diabetes: An autoimmune disease in which the immune system mistakenly attacks and destroys the beta cells of the pancreas that produce insulin. Without insulin, the body cannot use glucose from the blood for energy.
Type 2 Diabetes: The body becomes resistant to insulin or does not produce enough of it. It is often linked to excess body weight, physical inactivity, and aging, but genetics also plays a significant role.
2. Age of Onset
Type 1: Most often develops in childhood or adolescence but can occur at any age. Onset is usually sudden, with pronounced symptoms.
Type 2: Most common in adults over the age of 40, but increasingly seen in younger people and even children due to rising obesity rates and unhealthy habits. Symptoms develop gradually and often go unnoticed at first.
3. Insulin Production
Type 1: The pancreas completely stops producing insulin. Insulin therapy is essential for survival.
Type 2: The pancreas still produces insulin, but the body does not use it effectively (insulin resistance). In later stages, insulin production may drop significantly.
4. Treatment
Type 1:
Type 2:
- Lifestyle changes (diet, physical activity).
- Oral medications or injections to improve insulin sensitivity.
- In some cases – insulin.
-
5. Prevention
Type 1: Cannot be prevented, as it is caused by an autoimmune process.
Type 2: Can often be prevented or delayed with proper diet, regular exercise, and maintaining a healthy body weight.